VDRL Test full form is Venereal Disease Research Laboratory (VDRL) test. This is a nonspecific flocculation test which is used for the screening of syphilis. VDRL test is easy to perform and inexpensive, so it is commonly used in the screening of population for syphilis. Without some other evidence for the diagnosis of syphilis, a reactive nontreponemal test does not confirm Treponema pallidum infection.
The sample used are serum (plasma cannot be used) and Cerebrospinal Fluid (CSF). Acceptable CSF and serum specimen should not contain particulate matter that would interfere with reading test results.
Principle of VDRL Test
Non-treponemal antigen (Cardiolipin-Cholesterol-Lecithin) is used to detect the presence of “reagin antibodies” (IgM and IgG antibodies to lipoidal material released from damaged host cells as well as to lipoprotein-like material, and possibly cardiolipin released from the treponemes) in patient’s serum.
When the heat inactivated (to destroy complement) serum of a patient is reacted with freshly prepared non -treponemal antigen, flocculation reaction (antigen and antibody complex are suspended) occurs. The flocculation can be observed by using a microscope with a 10x objective and 10x eyepiece. Reactive VDRL test serum can be quantitated to obtain the titre of “reagin antibodies” by using serial double dilution method.
Purpose of VDRL Test
VDRL test is performed to detect or diagnose the Treponema pallidum infection. In case of pregnancy, the physician may ask to perform the VDRL test as a routine prenatal care check-up. In some cases, this test is needed for obtaining the marriage license or marriage certificate. Apart from its use to diagnose new infection, the physician may ask to perform the test to monitor the effectiveness of the treatment in patients who are found to be positive for syphilis. The anticardiolipin antibody titer may vary depending on the severity of the infection and effectiveness of the medication.
VDRL test also helps in screening congenital syphilis. In newborns, the test may sometimes give the false positive result. This is due to the transfer of antibodies from the infected mother to the child. In such case, the test should be repeated after a month to confirm the result.
VDRL Test Procedure
Patients’ serum is inactivated by heating at 56 degree Celsius for 30 minutes in a water bath to remove non-specific inhibitors (such as complement). The test can be performed both qualitatively and quantitatively. Those tests that are reactive by the Qualitative test are subjected to the Quantitative test to determine the antibody titres.
Qualitative Test:
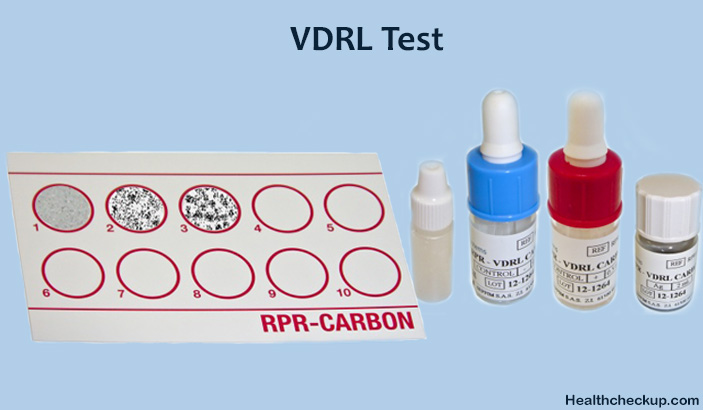
0.05 ml of inactivated serum is taken into one well. 1/60th ml (or 1 drop from 18 gauge needle) of the cardiolipin antigen is then added with the help of a syringe to the well and rotated at 180 rpm for 4minutes. Every test must be accompanied with known reactive and non-reactive controls. The slide is then viewed under low power objective of a microscope for flocculation. The reactive and non-reactive controls are looked first to verify the quality of the antigen. Depending on the size the results are graded as weakly reactive (W) or reactive(R). Reactive samples are then subjected to the quantitative test.
Qualitative Test:
This is performed to determine the antibody titres. The serum is doubly diluted in saline from 1in 2to 1:256 or more. 0.05 ml of each dilution is taken in the well and 1/60 ml of antigen is added to each dilution and rotated in a rotator. The results are then checked under the microscope. The highest dilution showing flocculation is considered as a reactive titre. Sometimes, due to the very high level of antibodies in the serum (prozone phenomenon), the qualitative test may be non-reactive. If the clinical findings are strongly suggestive of syphilis, a quantitative test may be directly performed on the serum specimen.
Requirements are patient’s serum, water bath, freshly prepared cardiolipin antigen, VDRL slide, mechanical rotator, pipettes, a hypodermic syringe with unbeveled needle and microscope. Known reactive and non-reactive serum controls are also required.
VDRL Antigen:
The cardiolipin antigen is an alcoholic solution composed of 0.03% cardiolipin, 0.21% lecithin and 0.9% cholesterol. The cardiolipin antigen must be freshly constituted each day of the test. The working antigen is an abuffered saline suspension of cardiolipin.
VDRL Slide:
This is a glass slide measuring 2 X 3 inch with 12 concave depressions, each measuring 16 mm in diameter and 1.75 mm deep.
Interpreting VDRL Test Results
VDRL test is positive in most cases of primary syphilis and are almost always positive in secondary syphilis. The titer of reagin antibodies decreases with effective treatment, so VDRL test can be used to determine the treatment response of syphilis.
The positive result is usually obtained one to two weeks after the primary lesion has appeared. Only during the late stage of primary syphilis, the test gives a 60-80% positive result. The test usually gives a strong positive result during the second phase of syphilis. After the second phase, the reactivity gradually decreases.
If the disease is diagnosed and treated in the primary phase itself, the antibody production gets suppressed and hence gives a non reactive result. On the other hand, treatments in the latent phase do not bring much effect on the antibody titer.
Limitations of the VDRL Test
A. False Positive VDRL Test Result
Reagin antibodies may be produced in response to nontreponemal diseases of an acute and chronic nature in which tissue damage occurs such as:
- Leprosy
- Hepatitis B
- Infectious Mononucleosis
- Various autoimmune Diseases
VDRL may be reactive in persons from areas where yaws are endemic. As a rule, residual titers from these infections will be <1:8.
Nontreponemal test titers of persons treated in latent or late stages of syphilis or who have become reinfected do not decrease as rapidly as do those from persons in the early stages of their first infection. In fact, these persons may remain “serofast,” retaining a low -level reactive titer for life.
B. False Negative VDRL Test
It can be seen because of prozone phenomenon (no flocculation due to antibody excess). In that case test serum has to be diluted further to obtain the zone of equivalence (where maximum flocculation of Ag-Ab occurs).
Since there are chances where the VDRL test may sometimes give a false positive result, the disease should be confirmed only by correlating with the clinical symptoms.
Medically Reviewed By

I am an experienced Medical/Scientific writer with a passion for helping people live a happy healthy life. My thirst for writing has followed me throughout the years – it is there when I wake up, lingering at the edges of my consciousness during the day, and teases me at night as I go to sleep.